You are here
Pelvi-ureteric Junction (PUJ) Obstruction
PUJ obstruction is a common problem seen in infants & children. In this condition, there is a partial obstruction (blockage) to urine flow from the kidney into the ureter (tube connecting the kidney to bladder). This results in swelling of the kidney (hydronephrosis). In severe cases, it can affect the functioning of the kidney. Routinely, this condition is diagnosed before birth itself. Some of there obstructions get better as the baby grows. However, if the blockage is causing severe swelling & pressure on the kidney, is affecting kidney function or causing infections, it needs to be surgically corrected.
The surgery for PUJ obstruction is called Pyeloplasty. In this operation, the blocked segment of the ureter is removed & the normal ureter joined to the pelvis of the kidney with fine sutures. A stent (called Double J stent) is inserted into the kidney with one end in the bladder to srain the urine while the stitches are healing. The stent is removed after about 6 weeks by endoscopy.
Laparoscopic Pyeloplasty in infants & children
Today all our pyeloplasty operations are sone by laparoscopy (key-hole surgery). Dr Chandrasekharam has performed over 280 laparoscopic pyeloplasties in infants & chiuldren which is the largest number in the country. More than half of these were in infants, including a 3 kg baby. In this, the same operation is done thru 3 small holes (each 3mm size) using special, delicate instruments. The operation currently takes about 1.5 hours & children are discharged in 2-3 days. Because of laparoscopy, this delicate operation is done under magnification (over 10 times magnified), is virtually painless & has excellent cosmetic result. The success of this operation in exoert hands is over 95%, & failures are uncommon. About 5% of children may have obstruction to both kidneys, & require surgery on both sides, one after the other.


PUJ obstructions: case scenarios
 Fig1: USG showing left hydronephrosis
Fig1: USG showing left hydronephrosis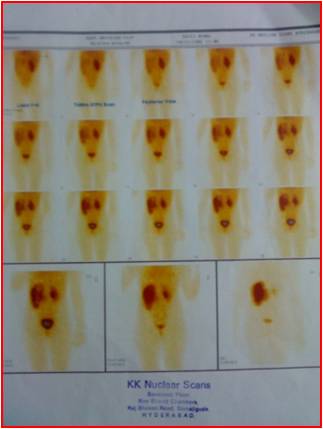 Fig 2: DTPA Renogram showing left PUJ obstruction with reduced function of left kidney
Fig 2: DTPA Renogram showing left PUJ obstruction with reduced function of left kidney
 Fig 3. Post operative USG shows significant reduction in hydronephrosis
Fig 3. Post operative USG shows significant reduction in hydronephrosis
 Fig 4. Post operative DTPA shows improved drainage (no obstruction) & improved function of Left Kidney
Fig 4. Post operative DTPA shows improved drainage (no obstruction) & improved function of Left Kidney